Abstract: Although many people take isolated nutrients as antioxidant supplements, they may not be getting the benefits they hope for. While isolated nutrients have powerful antioxidant abilities in vitro, they rarely have significant antioxidant benefits in vivo. High antioxidant containing foods have proven benefit in humans (in vivo) and high antioxidant effects in vitro as well. High antioxidant containing plants and other herbs are recommended for those interested in obtaining true antioxidant benefits.
Introduction
We live in a world where free radicals can come from many sources and contribute to deterioration of health. “Sources of free radicals include pollutants, drugs, metal ions, radiation, high intakes of polyunsaturated fatty acids, strenuous exercise, mitochondrial dysfunction and smoking. These may result in damage to membrane lipids, proteins, nucleic acids and carbohydrates, which can result in cancer, neurological diseases, lung diseases, diabetes, vascular diseases, autoimmune diseases, aging and eye diseases” [1]. Each day, each cell in the human body endures 104 hits from free radicals—that is about three hundred trillion hits to the body per day!
Antioxidants can inhibit oxidation by giving away an oxygen molecule without requiring much energy. Oxidation is the addition of oxygen or the removal of hydrogen and can be caused by free radicals. An antioxidant can slow down or even stop the chain reaction of oxidation by giving away an electron without changing its stability. Many believe that since real antioxidants can prevent free radical damage, that perhaps aging and various chronic conditions can, to some degree, be slowed down through the consumption of isolated antioxidant nutrients. Is this belief correct?
It is true that free radical damage to the skin contributes greatly to the aged appearance of the skin [2]. It is true that the consumption of high antioxidant containing foods is associated with a decreased risk of cancer and cardiovascular disease [3]. It is true that the consumption of high amounts of antioxidant containing foods is correlated with reduced risk of Alzheimer’s [4]. “Epidemiological studies have shown that consumption of fruits and vegetables is associated with reduced risk of chronic diseases. Increased consumption of fruits and vegetables containing high levels of phytochemicals has been recommended to prevent chronic diseases related to oxidative stress in the human body” [5].
Yet, it is also true that every large clinical trial, which has used isolated antioxidant supplements, has failed to show benefit for cancer and cardiovascular disease [6,7]. It is also true that in a recent trial, “The intake of {ISOLATED} vitamin C, beta-carotene and vitamin E supplements was not significantly associated with the risk of Alzheimer’s disease” [8]. “In two recent observational studies, higher dietary intakes of antioxidants {FOOD}, especially {FOOD} vitamin E, were found to be associated with a lower risk of Alzheimer’s disease. Neither study showed that supplemental {ISOLATED} vitamin E and vitamin C reduced the risk of Alzheimer’s disease. These findings suggest the involvement of other nutritional factors that may be involved in the reduced risk” [9].
(Note: Any words in this paper contained within {} are supplied by this investigator for clarification.)
Food vs. Isolated Form Nutrients
It should be understood that some who have concluded that antioxidant vitamins have little positive effect in vivo have normally failed to realize that the chemical forms of antioxidants used in these trials are often not quite the same as the form found in food.
Food antioxidants, be they vitamins, minerals, or concentrated herbs are superior to the commonly sold non-foods (note only officially recognized vitamins/minerals are listed below):
| Food Nutrient | Compared to USP Vitamin/Mineral Salt |
| Betacarotene | Provides much greater betacarotene diversity in blood [10] |
| Vitamin C | Over 15.6 times antioxidant effect [11] |
| Vitamin E | Up to 4.0 times the free radical scavenging strength [12] |
| Selenium | Nearly 2 times better retained [13] |
| Zinc | Better absorption, better form [14,15] |
Many have erroneously concluded that taking many times the quantity of isolated antioxidants will give the same effect as consuming food antioxidants. However, the differences are more than absorption or antioxidant effectiveness. Most isolated ‘antioxidant’ nutrients are chemically and structurally different from those found in foods and do not have the same effect in the human body.
“Beta-carotene has been found to have antioxidant effect in vitro…Whether {ISOLATED} beta-carotene has significant antioxidant effect in vivo is unclear” [16]. Carrots, a food high in betacarotene, do have high antioxidant ability [5,16]. Natural betacarotene, as found in foods, is composed of both all-trans and 9-cis isomers, while synthetic betacarotene is all-trans isomers [17]. Carrots, yellow and green leafy vegetables, and turmeric contain natural betacarotene along with multiple carotenoids. Natural betacarotene was found to significantly decrease serum conjugated diene levels for children exposed to high levels of irradiation, though it is not known if synthetic betacarotene would provide similar benefits [17].
Regarding isolated betacarotene, “The data presented provide convincing evidence of the harmful properties of this compound if given alone to smokers, or to individuals exposed to environmental carcinogens, as a micronutrient supplement” [7]. “The three beta-carotene intervention trials: the Beta Carotene and Retinol Efficacy Trial (CARET), Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study (ATBC), and Physician’s Health Study (PHS) have all pointed to a lack of effect of synthetic beta-carotene in decreasing cardiovascular disease or cancer risk in well-nourished populations. The potential contribution of beta-carotene supplementation to increased risk of lung cancer in smokers has been raised as a significant concern. The safety of synthetic beta-carotene supplements and the role of isomeric forms of beta-carotene (synthetic all-trans versus “natural” cis-trans isomeric mixtures)… have become topics of debate in the scientific and medical communities” [18]. Now, although the consumption of both synthetic betacarotene and food betacarotene raise serum vitamin A levels about the same, this obscures the fact that synthetic betacarotene tends to mainly increase serums all-trans betacarotene, while food betacarotene increases other forms as well [19].
It is possible that synthetic betacarotene can negatively affect vitamin E’s antioxidant ability as a clinical study found, “These results support earlier findings for the protective effect of a-tocopherol against LDL oxidation, and suggest that beta-carotene participates as a prooxidant in the oxidative degradation of LDL under these conditions. Since high levels of alpha-tocopherol did not mitigate the prooxidative effect of beta-carotene, these result indicate that increased LDL beta-carotene may cancel the protective qualities of alpha-tocopherol” [20]. In a consumer-directed publication, Stephen Sinatra (M.D.) observes, “Research has shown that high doses of synthetic beta-carotene—the kind found in many popular brands—may actually increase your risk for lung cancer. Because at high levels it can become prooxidative—exactly the opposite of what you want…I’ve seen harmful effects (such as serious vision loss) in people who have taken up to 80,000 IU of beta-carotene per day. The bottom line is: Less is more when it comes to beta-carotene. To be safe I recommend between 12,500 and 25,000 IU of beta-carotene per day from food sources such as carrots” [21].
In my opinion, betacarotene in carrots, however, is safer than even Dr. Sinatra suggests (there is about 12,000 i.u. of betacarotene in one raw carrot). The reason for this is because betacarotene in carrots is attached to lipoproteins which appear to aid in preventing toxicity. Isolated USP betacarotene, even if it allegedly comes from “natural” sources, simply does not have the attached lipoproteins or other potentially protective substances as found in foods like carrots.
Vitamin C in foods exists in at least two distinguishable forms with accompanying food factors [22]. Yet, regular ascorbic acid as well as mineral ascorbates are too incomplete to be properly called vitamin C as they do not contain both forms (i.e., they lack DHAA) and the accompanying food factors [22]! Foods contain both natural forms of vitamin C [22]! Also, foods containing vitamin C are normally less acidic than ascorbic acid.
In vitro studies found that food vitamin C has negative oxidative reductive potential [23], while isolated ascorbic acid had positive ORP [24]. Why is that so important? Because while antioxidants can stop free radical damage, only those substances with proper oxidative reductive potential can actually ‘clean up’ the damage that the free radicals cause. Please understand that “negative ORPs indicate active reducing power, which is immediately capable of antioxidant activity, whereas items with positive ORPs are not” [25]. It should be noted that the Merck Index shows that isolated ascorbic acid has positive redox potential [26].
A Cornell University study found that food vitamin C (as found in whole fruit) was 263 times more eftective as a free radical scavenger than isolated ascorbic acid [27]. This appears to be because fruits contain various naturally occurring phytochemicals are responsible for most of the antioxidant activity [27].
Although ascorbic acid has strong antioxidant effects in vitro, it is even possible isolated ascorbic acid has no in vivo antioxidant effects because “Despite epidemiological and some experimental studies, it has not been possible to show conclusively that higher than anti-scorbutic intake of {SYNTHETIC} vitamin C has antioxidant clinical benefit…{ISOLATED} Vitamin C may be a weak antioxidant in vivo, or its antioxidant actions may have no physiological role, or its role may be small. The oxidative hypothesis is unproven” [28]. Why should people take supplemental synthetic ascorbic acid when it is NOT been proven to have antioxidant effects in humans? On the other hand, high vitamin C containing foods do have proven in vitro and in vivo antioxidant effects [27,29].
One study found that food complex vitamin C had 492 micro moles per gram T.E. (Trolox equivalents) of hydrophilic ORAC (oxygen radical absorbance capacity) [30]—ORAC is essentially a measurement of the ability to quench free radicals (antioxidant ability)—while blueberries (one of the highest ORAC sources [11]) only had 195 micro moles per gram T.E. [30]—thus food complex vitamin C has 2.52 times the ORAC ability of blueberries. Vitamin C containing food has over 15.6 times the ORAC of isolated ascorbic acid [11] (food complex vitamin C is even higher). Actually, there are doubts that isolated ascorbic acid has any significant antioxidant effects in humans [28]. Food vitamin C is clearly superior for any interested in ORAC.
“Cross sectional and longitudinal studies show that the occurrence of cardiovascular disease and cancer is inversely related to vitamin C intake…the protective effects seen in these studies are attributable to fruit and vegetable {FOOD} intake…In general, beneficial effects of supplemental {SYNTHETIC} vitamin C have been noted in small studies, while large well controlled studies have failed to show benefit” [28]. The other quantitative is that in humans, “Plasma is completely saturated in doses of 400 mg and higher daily producing a steady-state plasma concentration of 80 mM…Tissues, however, saturate before plasma” [28]. De-emphasizing vitamin C containing foods by attempting to consume higher quantities of isolated ascorbic acid simply will not have the effects on plasma vitamin C levels, ORP, ORAC, or other health aspects that many consumers of isolated ascorbic acid hope it will [25,28].
So-called ‘natural’ ascorbic acid is made by fermenting refined sugar into sorbitol, then hydrogenating it until it turns into sorbose, then acetone (commonly referred to as nail polish remover) is added to break the molecular bonds which creates ascorbic acid [31]! How ‘natural’ is that?
While it is true that ascorbic acid has certain proven health benefits, no matter how much isolated ascorbic acid one takes orally:
1) It will never saturate plasma and/or tissue vitamin C levels significantly more than can be obtained by consuming sufficient vitamin C containing foods.
2) It will never have negative ORP, thus can never ‘clean-up’ oxidative damage like food vitamin C can.
3) It will never have the free radical fighting capacity of food vitamin C.
4) It will never contain DHAA (the other ‘half’ of vitamin C) or the promoting food factors.
5) It will never have the same effect on health issues, such as aging and cardiovascular disease as high vitamin C foods can.
6) It will not ever be utilized the way food vitamin C is.
7) It will always be a synthetic.
Although vitamin C, “can readily donate electrons to quench a variety of reactive free radical and oxidative species and is easily returned to its reduced state”, simply taking ascorbic acid C with two or three different antioxidants is not enough. Why? Because all free radical and oxidative substances do not get neutralized by all antioxidants.
Vitamin E “as found in foods is [d]-alpha tocopherol, whereas chemical synthesis produces a mixture of eight epimers” [32]. Natural vitamin E has recently been renamed to be called RRR-alpha-tocopherol whereas the synthetic has now been renamed to all-rac-alpha-tocopherol, though supplement labels rarely make this clear; on supplement labels d-alpha-tocopherol is generally ‘natural’, whereas dl-alpha-tocopherol is synthetic [32]. All acetate forms of vitamin E are synthetic. “The antioxidant function of vitamin E cannot be fulfilled by just any antioxidant” [12]. Natural RRR-alpha-tocopherol, which is found in food, has 1.7 – 4.0 times the free radical scavenging strength of the other tocopherols [12]. RRR-alpha tocopherol has 3 times the biological activity of the alpha-tocotrienol form, and synthetic vitamin E simply does not have the same biologic activity of natural vitamin E (some synthetic forms have only 2% of the biological activity of RRR-alpha-tocopherol) [12]. The biologic activity of vitamin E is based on its ability to reverse specific vitamin E-deficiency symptoms [12], therefore it is a scientific fact that, overall, synthetic vitamin E has less ability to correct vitamin E deficiencies than food vitamin E. There is an interesting reason for this, which is that the body regulates plasma vitamin E through a specific liver alpha-tocopherol transfer protein, whereas it has no such protein for other vitamin E forms [12]. Or in other words, the liver produces a protein to handle vitamin E found in Food, but not for the synthetic forms!
The body retains natural vitamin E 2.7 times better than synthetic forms [33]—it attempts to rid itself of synthetic forms as quickly as possible [33]. Vitamin E has been shown to reduce the risk of various cancers, coronary heart disease, cataract formation, and even air pollution [12,34]. It also is believed it may slow the aging process and decrease exercise-induced oxidative stress [12,34]. Artificial fats seem to increase the need for vitamin E [35]. Vitamin E content is highest in oils such as soy, but is also relatively high in rice bran [36].
Both chemical form and source of vitamin E may play a role as “chemically synthesized alpha-tocopherol is not identical to the naturally occurring form” [12]. Thus those who claim that a synthetic vitamin, even when it is in the same “chemical form” (it is never in the same actual form due to the presence of food constituents), is as good as one in a natural, food form, are simply overlooking the scientific facts about vitamins.
Food vitamin E, as found in specially grown rice, has been proven to have 12 micro moles per gram T.E. of lipophilic ORAC (oxygen radical absorbance capacity) [57]—ORAC is essentially a measurement of the ability to quench free radicals (antioxidant ability). It is interesting to note that so-called “natural” forms (like succinate) do not even work like food vitamin E. Even though many consider d-alpha-tocopherol as the best (isolated) natural form of vitamin E, the PDR notes, “d-Alpha-Tocopherol succinate itself has no antioxidant activity” [16] so why would anyone want that for their vitamin E supplement?
High dose isolated vitamin E can have pro-oxidant effects [37]. Jerome Block (M.D.) reports, “My research of the literature and my patients supports that this {ISOLATED} vitamin E supplement by itself does not supply adequate antioxidant protection…If one takes the {ISOLATED} commercial form of vitamin E…there is evidence that the effect of the antioxidant is not present…vitamin E found in foods is much more effective than the single alpha-tocopherol supplements…Although vitamin E has an excellent safety record, studies show that alpha-tocopherol alone…has been pro-oxidant rather than antioxidant” [38]. Food vitamin E, which has proven antioxidant abilities [12], is clearly superior to the isolated versions.
Selenium is a mineral with antioxidant abilities and is also “a necessary mineral for the production of antioxidants in the body” [27]. The three most common forms of selenium in supplements are sodium selenite, seleniomethionine, and food selenium. The predominant form of selenium found in the body and in food selenium is selenocysteine [39]. Human research suggests that food selenium is less toxic than industrial/mineral salt form [39].Food selenium (which is normally a specially grown yeast food) should not be confused with yeasts which have been simply fortified with sodium selenite, which can be quite toxic. Sodium selenite is not a food, but is the result of combining sodium hydroxide and selenious acid; sodium selenite is commonly used to remove green color from glass during glass manufacturing [26]. Why would anyone want to take that as part of their antioxidant supplement?
One study using 247 mcg/day of high-selenium yeast found that plasma selenium levels were 2-fold higher than baseline values after 3 and 9 months and returned to 136% of baseline after 12 months, whereas there was a 32% increase in blood glutathione levels also seen after 9 months. This change coincided with a 26% decrease in protein-bound glutathione and a 44% decrease in the ratio of protein-bound glutathione to blood glutathione. The changes in glutathione and protein-bound glutathione were highly correlated with changes in plasma selenium levels and were believed to reflect a reduction in oxidative stress [40].
It has been reported that food selenium seems to reduce toxicity associated with cisplatin chemotherapy [41], hence many people take it when undergoing conventional cancer treatments. Furthermore, Larry Clark, Ph.D. and others have found that selenium in yeast appears to reduce risk of certain cancers [42]. Julian Whitaker, M.D. reports, “The best absorbed form of selenium, and the one used by Dr. Clark’s research, is high-selenium yeast” [42].
Food selenium is about twice as well retained as non-food forms [13,40].
Zinc is an important component of superoxide dismutase (see below). “Dietary zinc has potent antioxidant and anti-inflammatory properties” [43]. Additionally, “Poor zinc nutrition may be an important risk factor in oxidant release and the development of DNA damage and cancer. Approximately 10% of the United States population ingests <50% of the recommended daily allowance for zinc, a cofactor in proteins involved in antioxidant defenses, electron transport, DNA repair and p53 protein expression” [44].
High zinc-containing foods include wheat bran, beef, miso, spinach, mushrooms, alfalfa sprouts, brewer’s yeast, turkey, lamb, bean sprouts, tofu, and to a lessor degree in whole wheat bread [45] (shellfish also contains zinc, but this researcher cannot recommend that as a source). Zinc in unleavened whole wheat bread is less bioavailable than zinc in whole wheat bread leavened with yeast [15]; enzymatically-processed food grade yeast seems to contain some of the most bioavailable food zinc. Research also suggests that certain food forms of zinc are better absorbed and retained than non-food forms [15,16].
Superoxide Dismutase
Superoxide dismutase (S.O.D.) is naturally found in foods such as nutritional yeast and barley green. It is not considered to be an essential nutrient, nor is it an herb (though it does exist in plants). However, S.O.D. “is one of the most important enzymes that functions as a cellular antioxidant…The absence of this enzyme is lethal” [46]. Although S.O.D. (like glutathione, lipoic acid, etc.) is not a vitamin/mineral it is listed here separately because it may be the single most important antioxidant (it is possible that some other antioxidant will take over that role, but more studies appear to have been published about S.O.D. than possibly any other non-vitamin, non-mineral antioxidant).
“It protects intracellular components from oxidative damage, converting the superoxide ion to hydrogen peroxide” [47]. S.O.D. appears to be able to prevent activation of “phospholipase A2 and proanoid synthesis by scavenging free radicals, thereby reducing lipid peroxidation products” [48]. It is a powerful free radical scavenger, which has been clinically shown to protect the brain, heart, liver, lungs, kidneys, skin, muscles, penis, nerves, and spinal cord from ischemic injury [48].
S.O.D. has been shown to inhibit articular tissue damage associated with osteoarthritis [49], decreases lipid peroxidation in damaged skin cells [50], protect against late radiation-induced tissue injury [51], improves clinical symptoms associated with Bechet’s syndrome [52], helps protect the retina [53], helps protect against iron toxicity [54], inhibits vasogenic brain edema after brain injury [55], increases flu survival rates in mice [56], plays a role in bacterial defense [57], helps normalize blood pressure [58,59] helpful for cardiovascular problems [48,60,61], reduces LDL oxidation involved in atherosclerosis [61], is reduced in Alzheimer’s patients [62], improves sperm motility [63], and even helped patients with TMJ who did not respond to traditional therapy [64]; there over a thousand recent (within the last 5 years) peer-reviewed papers on S.O.D. High levels of S.O.D. have been associated with reduced growth of Candida albicans [65]. It is often sold in a “purified” version (from animal products) as an antiaging product [44]; S.O.D. seems to have “antiaging” properties [48]. Ingestion of polyethylene glycol-conjugated superoxide dismutase is not as effective as CuZn (copper/zinc) superoxide dismutase [66,67]. CuZn superoxide dismutase, along with Mn superoxide dismutase [68] exists naturally, in foods such as nutritional yeast (Saccharomyces cerevisiae).
Antioxidant Herbs
There are many antioxidant plants and other herbs. All antioxidants in plants and herbs exist in their natural food forms, hence (unless isolated) are true antioxidants. The following list is not exhaustive (and intentionally does not include green tea as the caffeine it contains is a problem for some):
Barley Grass Concentrate contains a variety of antioxidant substances, including natural S.O.D. (see Superoxide dismutase earlier in this paper) which is also able scavenge reactive oxygen species [69,70]. “Research at the University of California Davis has demonstrated that a flavonoid in barley grass known as 2-0-glycosylisovitexin (2-0-GIV) is a potent antioxidant which is more powerful than other antioxidants in protecting against fat oxidation (lipid peroxidation) in human cells’ [71]. Others state, “the major flavonoid antioxidants in young green barley leaves are in fact the flavone-C-glycosides, saponarin and lutonarin” [72]. Barley grass (like wheat grass and other green plants) also contains chlorophyll, which has antioxidant ability [15].
Carrots provide betacarotene (see Betacarotene earlier in this paper) and other antioxidant carotenoids. Carrots also contain “xanthophyll, a very powerful anticancer phytochemical” [71]. Carrots are one the vegetables with high total antioxidant activity [5].
Citrus Fruits, which are common in Western diets, contain a variety of antioxidants such as flavonoids [15] and food vitamin C (see Vitamin C above). Citrus fruits have been shown to have significant antioxidants in vivo (and in vitro) [5]. Pink grapefruit is a source of lycopene (as are tomatoes) [15]. The peel and pulp of citrus has more of the flavonoid hesperidian than the juice [15].
Eleuthro Root, which was formerly called Siberian Ginseng, is an adaptagen, which means that it helps the body deal with various forms of stress [73]. It has been found to have “strong antioxidant against scavenging on DPPH free radical and also ethyl acetate fractionation exhibited high antilipid peroxidative activities. In the cytotoxic effects were evaluated on seven human cancer cell lines, the values of 50% growth inhibition (GI(50)) were mostly below 30 microg/ml for crude extracts to be considered as significantly active” [74]. A Russian study found that it had strong antioxidant abilities [75].
Ginger Root has constituents with antioxidant effects and can improve peripheral circulation [73]. Specifically it has at least “four shogaols that protect IMR32 human neuroblastoma and normal human umbilical vein endothelial cells from beta-amyloid(25 – 35) insult at EC50 = 4.5 – 81 microM” [76]. Ginger is one of the plants that contain the most antioxidants [77].
Ginkgo Leaf contains about 40 different bioflavonoids, including proanthocyanidins (see Grape Seed/Skin extract below) and quercetin, that “act as free radical scavengers” [73]. “Quercitin is a phenolic antioxidant that and has been shown to inhibit lipid peroxidation” in vitro, but it may need food substances to be an effective antioxidant in vivo [15]. “Cerebral insufficiency many cause anxiety and stress, memory, concentration, and mood impairment, and hearing disorders, all of which may benefit from ginkgo therapy” [73]. “Recent studies conducted with various molecular, cellular and whole animal models have revealed that leaf extracts of Ginkgo biloba may have anticancer (chemopreventive) properties that are related to their antioxidant, anti-angiogenic and gene-regulatory actions. The antioxidant and associated anti-lipoperoxidative effects of Ginkgo extracts appear to involve both their flavonoid and terpenoid constituents…In humans, Ginkgo extracts inhibit the formation of radiation-induced (chromosome-damaging) clastogenic factors and ultraviolet light-induced oxidative stress – effects that may also be associated with anticancer activity. Flavonoid and terpenoid constituents of Ginkgo extracts may act in a complementary manner to inhibit several carcinogenesis-related processes, and therefore the total extracts may be required for producing optimal effects” [78]. Ginkgo biloba extracts, “could reduce cytokine-stimulated endothelial adhesiveness by downregulating intracellular reactive oxygen species formation, nuclear factor-kappaB and activator protein 1 activation, and adhesion molecule expression in HAECs, supporting the notion that the natural compound Ginkgo biloba may have potential implications in clinical atherosclerosis disease” [79].
Grape Seed/Skin Extract contains a variety of antioxidant substances and is over 90% proanthocyanidins, which are a type of bioflavonoid with powerful free radical fighting ability [73]. “Oligomeric proanthocyanidins, naturally occurring antioxidants widely available in fruits, vegetables, nuts, seeds, flowers and bark, have been reported to possess a broad spectrum of biological, pharmacological and therapeutic activities against free radicals and oxidative stress. We have assessed the concentration- or dose-dependent free radical scavenging ability of a novel IH636 grape seed proanthocyanidin extract (GSPE) both in vitro and in vivo models, and compared the free radical scavenging ability of GSPE with {ISOLATED} vitamins C, E and beta-carotene. These experiments demonstrated that GSPE is highly bioavailable and provides significantly greater protection against free radicals and free radical-induced lipid peroxidation and DNA damage than vitamins C, E and beta-carotene. Oxidative tissue damage was determined by lipid peroxidation and DNA fragmentation, while apoptotic cell death was assessed by flow cytometry. GSPE provided significantly better protection as compared to vitamins C and E, singly and in combination. GSPE also demonstrated excellent protection against acetaminophen overdose-induced liver and kidney damage by regulating bcl-X(L) gene, DNA damage and presumably by reducing oxidative stress. GSPE demonstrated excellent protection against myocardial ischemia-reperfusion injury and myocardial infarction in rats. GSPE was also shown to upregulate bcl(2) gene and downregulate the oncogene c-myc. Topical application of GSPE enhances sun protection factor in human volunteers, as well as supplementation of GSPE ameliorates chronic pancreatitis in humans. These results demonstrate that GSPE provides excellent protection against oxidative stress and free radical-mediated tissue injury” [80]—it should be noted that this study compared against isolated (non-food) vitamins and isolated betacarotene. Interestingly it is believed that “grape-skin extract may have a sparing effect on vitamin C” in human plasma [81]. Grape seeds, but mainly grape skin, contains resveratrol which has antioxidant abilities and may be “associated with a reduced incidence of cardiovascular disease and a reduced incidence of cancer” [15]. Resveratrol is prized by many for its anti-aging properties and “has recently been found to possess glutathione-sparing activity” [15].
Kudzu Root contains a powerful antioxidants, including an isoflavone known as puerarin [82]. “Kudzu was found to be an effective adsorbent for basic dye colour removal” [83]. Kudzu and puerarin are being investigated for their apparent ability to suppress alcohol desire for alcoholics [84]; it is also being investigated for its ability to glucose control for diabetics. One study found that kudzu in crude form appears to have greater antioxidant effects than isolated puerarin [85].
Milk Thistle Seed contains silymarin, which is a polyphenolic antioxidant flavonoid [17]. “Silymarin is an antihepatotoxic substance isolated from fruits of Silybum marianum. Possibly due to their antioxidant and membrane stabilizing properties, the compounds have been shown to protect different organs and cells against a number of insults” [86]. Silybinin is a component of silymarin and has been shown to reduce lipid peroxidation [87]. Furthermore, “silibinin inhibits the growth of human prostate cancer cells (PCA) both in vitro and in vivo” [88].
Rosemary Leaf contains flavonoid antioxidants [71] and can “increase detoxification of carcinogens” in certain instances [73]. It contains such flavonoids as cirismarin, diosmin, hesperidin, homoplantiginin, and phegopolin [89]. Topically, rosemary is used to promote wound healing and as an analgesic for myalgias and neuralgias [89].
Saccharomyces cerevisiae, also known as nutritional yeast, contains antioxidants such as S.O.D. (see above) and glutathione (actually most isolated glutathione comes from fermented yeast [15]). Certain food antioxidant nutrients grown in Saccharomyces cerevisiae, such as zinc and selenium have been shown to have higher antioxidant effects and/or better absorption than the isolated mineral salt versions that are commonly sold [13,14,35,43,45]. Saccharomyces cerevisiae also naturally contains protein chaperones, which are essential for mineral absorption. Saccharomyces cerevisiae also stimulates phagocytosis [89]. The bioavailability of coenzyme q10 (a substance with antioxidant properties) is enhanced when it is in a media containing Saccharomyces cerevisiae [90].
Schisandra Fruit “has pronounced liver protective effects” [73] and strong antioxidant activity [91]. Schisandra contains at least 9 dibenzocyclooctene lignans, “Seven of the 9 lignans (1 mM) inhibited iron/cysteine-induced lipid peroxidation (malondialdehyde, MDA, formation)…The actions of the 7 lignans were much more potent than vitamin E at the same concentration of 1 mM. Among the lignans, schisanhenol was the most active one. This compound also prevented the decrease of membrane fluidity of liver microsomes induced by iron/cysteine. The results indicated that seven of the lignans such as schisanhenol have anti-oxidant activities” [91].
Tomatoes are a source of lycopene [15] and food vitamin C [21]. “Lycopene is a member of the carotenoid family…[and] is responsible for the red color of red tomatoes” [15]. “In vitrostudies have demonstrated that lycopene has the highest antioxidant activity of all the carotenoids” [15]. Yet, it does not seem to have the same effect in vivo as tomatoes themselves do. One recent study that compared tomatoes to isolated lycopene found that tomatoes inhibited prostate carcinogenesis but that lycopene did not [92].
Turmeric Root contains curcuminoids which have antioxidant and cancer-inhibiting properties [73]. Many “laboratory studies have identified a number of different molecules involved in inflammation that are inhibited by curcumin including phospholipase, lipooxygenase, cyclooxygenase 2, leukotrienes, thromboxane, prostaglandins, nitric oxide, collagenase, elastase, hyaluronidase, monocyte chemoattractant protein-1 (MCP-1), interferon-inducible protein, tumor necrosis factor (TNF), and interleukin-12 (IL-12)” [93].
Water Thyme is one of the most mineral-dense foods and contains nutritional antioxidants, including vitamin C (see Vitamin C above) and chlorophyll. It is sometimes included in food antioxidant formulas.
Conclusion
Herbs and plants containing antioxidants offer unique benefits, which have not been synthetically duplicated.
Actually, no matter how much synthetic vitamins or industrially-processed rock ‘nutrients’ one takes orally, they will:
1) Never be a truly complete nutrient source.
2) Never replace all the functions of food/herbal vitamins and minerals.
3) Always be unnatural substances to the body.
4) Always strain the body by requiring that it detoxify or somehow dispose of their unnatural structures/chemicals.
5) Never be utilized, absorbed, and retained the same as food/herbal nutrients.
6) Not be able to prevent advanced protein glycation end-product formation the same as food/herbal nutrients.
7) NEVER BE ABLE TO HAVE THE PROVEN ANTIOXIDANT EFFECTS THE SAME AS FOOD NUTRIENTS.
8) Always be industrial products.
9) Always be composed of petroleum-derivatives, hydrogenated sugars, and/or industrially-processed rocks.
10) Never build optimal health the same as food nutrients.
The standards of naturopathy agreed to in 1947 (at the Golden Jubilee Congress) included the statements, “Naturopathy does not make use of synthetic or inorganic vitamins…Naturopathy makes use of the healing properties of…natural foods, organic vitamins” [94]. Even back in the 1940s, professionals interested in natural health recognized the value of food, over non-food, vitamins.
Although many studies have demonstrated that isolated nutrients such as betacarotene, ascorbic acid, and alpha-tocopherol do have significant antioxidant effects in test tubes (in vitro), more recent research has raised serious questions as to whether these chemical isolates have significant antioxidant effects in humans (in vivo) [15,23,33]. Furthermore, in 1999 the Nobel prize for medicine was awarded to Gunter Blobel who discovered that nutritional minerals need protein chaperones for absorption. Such protein chaperones do not exist in mineral salt forms which are commonly included in ‘antioxidant’ or multivitamin formulas. Protein chaperones do, of course, exist in foods such as Saccharomyces cerevisiae [95,96].
While it is known that diets focused on foods high in antioxidants can help prevent cancers [3], synthetic antioxidants appear to be so ineffective that they may actually increase cancer risk [6]. Additionally, regarding cancer and other diseases, “The available evidence points to the benefits of food-derived antioxidants, but more evidence is needed before {ISOLATED} antioxidant…supplementation can be routinely recommended” [97]. “A predominantly plant-based diet reduces the risk for development of several chronic diseases. It is often assumed that antioxidants contribute to this protection, but results from intervention trials with single antioxidants administered as supplements quite consistently do not support any benefit. Because dietary plants contain several hundred different antioxidants” [77], it makes sense to consume food antioxidants and not individual, isolated ones.
Although some scientists think isolated nutrients have questionable and even negative effects, “It is doubtful that antioxidant-rich foods would have a negative impact on brain aging” [9]—or anything else for that matter. Humans are supposed to eat foods and not consume isolated USP nutrients (even if they are called ‘natural’ and even if they are called ‘antioxidants’). Since all free radical and oxidative substances do not get neutralized by all antioxidants, it makes sense to consume a variety of plants and/or antioxidant containing herbs—plants which contain hundreds of antioxidant compounds [15,77,89].
“Unfortunately, a single purified substance will not always have the same antioxidant activity, nor provide the same clinical benefits as…combinations occurring in natural extracts” [98]. Some of these ‘purified’ substances have been shown to sometimes have pro-oxidant instead of antioxidant effects [19,20,32,33].
Why would anyone want to take isolated ‘antioxidants’ instead of foods or those antioxidant formulas which are only composed of 100% food?
References:
[1]Lachance PA, Nakat Z, Jeong W-S. Antioxidants: An Integrative Approach. Nutr, 2001;17:835-838
[2] Kagan VE, Kisin ER, Kawai K, Serinkan BF, Osipov AN, Sertbinova EA, Wolinsky I, Shvedova AA. Towards mechanism-based antioxidant interventions. Ann NY Acad Sci 2002;959:188-198
[3] Francheschi S, Parpinel M, La Vecchia C, Favero A, Talamini R, Negri E. Role of different types of vegetables and fruit in the prevention of cancer of the colon, rectum, and breast. Epidemiology 1998;9(3):338-341
[4] Engelhart MJ, Geerlings MI, Ruitenberg A, et al. Dietary Intake of Antioxidants and Risk of Alzheimer Disease. JAMA 2002;287(24):3223-3229
[5] Chu YF, Sun J, Wu X, Liu RH. Antioxidant and antiproliferative activities of common vegetables. J Agric Food Chem. 2002;50(23):6910-6916
[6] Rautalahti M, Huttunen J. Antioxidants and carcinogenesis. Ann Med 1993;25:435-441
[7] Paolini M, Abdel-Rahman SZ, Sapone A, Pedulli GF, Perocco P, Cantelli-Forti G, Legator MS. Beta-carotene: a cancer chemopreventive agent or a co-carcinogen? Mutat Res. 2003;543(3):195-200
[8] Morris MC, Evans DA, Bienias JL, et al. Dietary Intake of Antioxidant Nutrients and the Risk of Incident Alzheimer Disease in a Biracial Community Study. JAMA 2002;287(24):3230-3237
[9] Foley DJ, White LR. Dietary Intake of Antioxidants and Risk of Alzheimer Disease: Food for Thought. JAMA, 2002;287(24):3261-3263
[10] van het Hof KH, Gartner C, Wiersma A, Tijburg LB, Weststrate JA. Comparison of the bioavailability of natural palm oil carotenoids and synthetic beta-carotene in humans. J Agric Food Chem. 1999;47(4):1582-6
[11] Williams D. ORAC values for fruits and vegetables. Alternatives, 1999;7(22):171
[12] Traber MG. Vitamin E. In Modern Nutrition in Health and Disease, 9th ed. Williams & Wilkins, 1999:347-362
[13] Biotechnology in the Feed Industry. Nottingham Press, UK, 1995: 257-267
[14] Andlid TA, Veide J, Sandberg AS. Metabolism of extracellular inositol hexaphosphate (phytate) by Saccharomyces cerevisiae. Int J. Food Microbiology. 2004;97(2):157-169
[15] King JC, Cousins RJ. Zinc. In Modern Nutrition in Health and Disease, 10 th ed. Lipponcott Williams & Wilkins, Phil., 2006:271-285
[16] Hendler S, Rorvik D ed. PDR for Nutritional Supplements. Medical Economics, Montvale (NJ), 2001
[17] Ben-Amotz A, et al. Effect of natural beta-carotene supplementation in children exposed to radiation from the Chernobyl accident. Radiat Environ Biophys 1998;37:187-193
[18] Patrick L. Beta-carotene: the controversy continues. Altern Med Rev. 2000;5(6):530-45
[19] Ben Amotz; van het Hof KH, Gartner C, Wiersma A, Tijburg LB, Westrate JA. Comparison of the bioavailability of natural palm oil carotenoid and synthetic beta-carotene in humans. J Agric Food Chem, 1999;47(4):1582-1586
[20] Bowen HT, Omaye ST. Oxidative changes associated with beta-carotene and alpha-tocopherol enrichment of human low-density lipoproteins. J Am Coll Nutr. 1998;17(2):171-179
[21] Sinatra S. Consumer Alert: Don’t Touch this Button, 2003:34-35
[22] Jacob RA. Vitamin C. In Modern Nutrition in Health and Disease, 9th ed. Williams & Wilkins, Balt.,1999:467-483
[23] Thiel R. ORP Study on Durham-produced Food Vitamin C for Food Research LLC. Doctors’ Research Inc., Arroyo Grande (CA), February 17, 2006
[24] Thiel RJ. Natural vitamin C is better than isolated ascorbic acid. ANMA Monitor, 1999;3(3):5-7
[25] Thiel R.J, Fowkes S.W. Can cognitive deterioration associated with Down syndrome be reduced? Medical Hypotheses, 2005; 64(3):524-532
[26] Budavari S, et al. The Merck Index, 12th ed. Merck & Co., Whitehouse Station (NJ), 1996
[27] Eberhardt MV, Lee CY, Liu RH. Antioxidant activities of fresh apples. Nature 2000;405:903-904
[28] Sebastian J, et al. Vitamin C as an antioxidant: evaluation of its role in disease prevention. J Am Coll Nutr, 2003;22(1):18-35
[29] Proteggente AR, et al. The antioxidant effect activity of regularly consumed fruit and vegetables reflect their phenolic and vitamin C composition. Free Radic Res, 2002;36(2):217-233
[30] ORAC Test by Brunswick Laboratories, Wareham (MA), February 2006
[31] Vitamin-Mineral Manufacturing Guide: Nutrient Empowerment, volume 1. Nutrition Resource, Lakeport (CA), 1986
[32] Farrel PM, Robert RJ. Vitamin E. In Modern Nutrition in Health and Disease, 8th ed. Lea & Febiger, Phil.;1994:326-341
[33] Traber MG, Elsner A, Brigelius-Flohe R. Synthetic as compared with natural vitamin E is preferentially excreted as alpha-CEHC in human urine: studies using deuterated alpha-tocopherol acetates. FEBS Letters, 1998;437:145-148
[34] An Overview of Vitamin E Efficacy. VERIS Research Information Service, November 1998
[35] Schlagheck TG, et al. Olestra’s effect on vitamins D and E in humans can be offset by increasing dietary levels of these vitamins. J Nutr,1997;127(8):1666S-1685S
[36] Rice bran, crude. USDA National Nutrient Database for Standard Reference, Release 18, 2005
[37] Ikemoto M, Okamura Y, Kano M, Hirasaka K, Tanaka R, Yamamoto T, Sasa T, Ogawa T, Sairyo K, Kishi K, Nikawa T. A relative high dose of vitamin E does not attenuate unweighting-induced oxidative stress and ubiquitination in rat skeletal muscle. J Physiol Anthropol Appl Human Sci. 2002;21(5):257-263
[38] Block J. To E or not to E, that is the question. Orig Internist 2003;10(3):23
[39] Levander OA, Burk RF. Selenium. In Modern Nutrition in Health and Disease, 8th ed. Lea & Febiger, Phil., 1994:242-263
[40] El-Bayoumy K, Richie JP Jr, Boyiri T, Komninou D, Prokopczyk B, Trushin N, Kleinman W, Cox J, Pittman B, Colosimo S. Influence of Selenium-Enriched Yeast Supplementation on Biomarkers of Oxidative Damage and Hormone Status in Healthy Adult Males: A Clinical Pilot Study. Cancer Epidemiol Biomarkers Prev. 2002;11:1459-1465
[41] Ya-Jun, H, et al. The protective role of selenium on the toxicity of cisplatin-contained chemotherapy regimen in cancer patients. Bio Trace Element Res, 1997;56:331-341
[42] Whitaker J. Minerals, part 1: Cut your cancer risk with selenium. Health & Healing, 1999;9(4):6-8
[43] Meerarani P, Reiterer G, Toborek M, Hennig B. Zinc modulates PPARgamma signaling and activation of porcine endothelial cells. J Nutr. 2003 Oct;133(10):3058-3064
[44] Ho E, Courtemanche C, Ames BN. Zinc deficiency induces oxidative DNA damage and increases p53 expression in human lung fibroblasts. J Nutr. 2003 Aug;133(8):2543-2548
[45] Whitney EN, Hamilton EMN. Understanding Nutrition, 4th ed. West Publishing, NY, 1987
[46] Thomas JA. Oxidative stress, oxidant defense, and dietary constituents. In Modern Nutrition in Health and Disease, 8th ed. Lea & Febiger, Phil.;1994:501-512
[47] Turnland JR. Copper. In Modern Nutrition in Health and Disease, 8th ed. Lea & Febiger, Phil.,1994:231-241
[48] Null G. Superoxide Dismutase. In The Clinician’s Handbook of Natural Healing. Kensington Books, New York, 1997:137-144
[49] Hoedt-Schmidt S, et al. Histomorphological studies on the effect of recombinant human superoxide dismutase in biochemically induced osteoporosis. Pharmacol,1993;47(4):252-260
[50] Okumura K, Nishiguchi K, Tanigawa Y, Mori S, Iwakawa S, Komada F. Enhanced anti-inflammatory effects of Cu, Zn-superoxide dismutase delivered by genetically modified skin fibroblasts in vitro and in vivo. Pharm Res,1997;14(9):1223-1227
[51] Delanian S, Baillet F, Huart J, Lefaix JL, Maulard C, Housset M. Successful treatment of radiation-induced fibrosis using liposomal Cu/Zn superoxide dismutase: clinical trial. Radiother Oncol,1994;32(1):12-20
[52] Merit J, et al. Preliminary study of the therapeutic effect of superoxide dismutase in 7 cases of Bechet’s syndrome. C R Acad Sci III,1986;302(7):243-246
[53] Behndig A, Svensson B, Marklund SL, Karlsson K. Superoxide dismutase isoenzymes in the human eye. Invest Opthalmol Vis Sci,1998;39(3):471-475
[54] Wi’snicka R, Krzepiko A, Wawryn J, Krawiec Z, Bili’nski T. Protective role of superoxide dismutase in iron toxicity in yeast. Biochem Mol Biol Int,1998;44(3):635-641
[55] Chan PH, et al. Protective effects of liposome-entrapped superoxide dismutase on posttraumatic brain injury. Ann Neur,1987;21(6):540-547
[56] Sharonov BP, et al. The effective use of superoxide dismutase from human erythrocytes in the late stages of experimental influenza infection. Vopr Virusol,1991;36(6):477-480
[57] San Mateo LR, Hobbs MM, Kawula TH. Periplasmic copper-zinc superoxide dismutase protects Haemophilus ducreyi from exogenous superoxide. Mol Microbiol,1998;27(2):391-404
[58] Zhang XM, Ellis EF. Effects of superoxide dismutase decreases mortality, blood pressure, and cerebral blood flow responses induced by acute hypertension in rats. Chung Kuo Yao Li Hsueh Pao,1990;11(4):324-328
[59] Przyklenk K, Kloner RA. Superoxide dismutase plus catalase improve contractile function in the canine model of the stunned myocardium. Circulatory Res,1986;58(1):148-156
[60] Nelson SK, Bose SK, McCord JM. The toxicity of high dose superoxide dismutase suggests that superoxide can both initiate and terminate lipid peroxidation in the reperfused heart. Free Radic Biol Med,1994;16(2):195-200
[61] Wang P, et al. Overexpression of human copper, zinc-superoxide dismutase (SOD1) prevents postischemic injury. Proc Natl Acad Sci U S A,1998;95(8):4556-4560
[62] De Deyn PP, et al. Superoxide dismutase activity in cerebrospinal fluid of patients with dementia and some other neurological disorders. Alzheimer Dis Assoc Discord,1998;12(1):26-32
[63] Kobayshi T, Miyazaki T, Natori M, Nozawa S. Protective role of superoxide dismutase in human sperm motility: superoxide dismutase activity and lipid peroxide in human seminal plasma and spermatozoa. Hum Reprod,1991;6(7):987-991
[64] Lin Y, et al. Use of superoxide dismutase (SOD) in patients with temporomandibular joint dysfunction. Intl J Oral Maxillofac Surg,1994;23(6pt2):428-429
[65] Romandini P, Bonotto C, Bertoloni G, Beltramini M, Salvato B. Superoxide dismutase, catalase and cell dimorphism in Candida albicans cells exposed to methanol and different temperature. Comp Biochem Physiol Pharm Toxicol Endocrinol,1994;108(1):53-57
[66] Haun SE, Kirsch JR, Helfaer MA, Kubos KL, Traystman RJ. Polyethylene glycol-conjugated superoxide dismutase fails to augment brain superoxide dismutase activity in piglets. Stroke,1991;22(5):655-659
[67] Tibell L, Aasa R, Marklund SL. Spectral and physical properties of human extracellular superoxide dismutase: a comparison with CuZn superoxide dismutase. Arch Biochem Biophys, 1993;304(2):429-433
[68] Turi TG, Kalb VF, Loper JC. Cytochrome P450 lanosterol 14 alpha-demethylase (ERG11) and manganese superoxide dismutase (SOD1) are adjacent genes in Saccharomyces cerevisiae. Yeast,1991;7(6):627-630
[69] Cremer L, Herold A, Avram D, Szegli G. A purified green barley extract with modulatory properties upon the TNF alpha and ROS released human specialised cells isolated from RA patients. Roum Arch Microbiol Immunol 1998;57(3-4):231-242
[70] Yu YM, Chang WC, CHang CT, Hsieh CL, Tsai CE. Effects of young barley leaf extract and antioxidative vitamins on LDL oxidation and free radical scavenging activities in type 2 diabetes. Diabetes Metab 2002;28(2):107-114
[71] Duarte A. Health Alternatives. Megasystems, Morton Grove (IL), 1995
[72] Markham KR, Mitchell KA. The mis-identification of the major antioxidant flavonoids in young barley (Hordeum vulgare) leaves. Z Naturforsch [C] 2003;58(1-2):53-56
[73] DerMarderosian A, editor. The Review of Natural Products, 1st ed. Facts and Comparisons, St. Louis, 2001
[74] Yu CY, Kim SH, Lim JD, Kim MJ, Chung IM. Intraspecific relationship analysis by DNA markers and in vitro cytotoxic and antioxidant activity in Eleutherococcus senticosus. Toxicol In Vitro. 2003;17(2):229-236
[75] Bol’shakova IV, Lozovskaia EL, Sapezhinskii II. Antioxidant properties of a series of extracts from medicinal plants. Biofizika. 1997 Mar-Apr;42(2):480-483
[76] Kim DS, Kim DS, Oppel MN. Shogaols from Zingiber officinale protect IMR32 human neuroblastoma and normal human umbilical vein endothelial cells from beta-amyloid(25-35) insult. Planta Med. 2002;68(4):375-376
[77] Halvorsen BL, Holte K, Myhrstad MC, Barikmo I, Hvattum E, Remberg SF, Wold AB, Haffner K, Baugerod H, Andersen LF, Moskaug O, Jacobs DR Jr, Blomhoff R. A systematic screening of total antioxidants in dietary plants. J Nutr. 2002 Mar;132(3):461-471
[78] DeFeudis FV, Papadopoulos V, Drieu K. Ginkgo biloba extracts and cancer: a research area in its infancy. Fundam Clin Pharmacol. 2003;17(4):405-417
[79] Chen JW, Chen YH, Lin FY, Chen YL, Lin SJ. Ginkgo biloba Extract Inhibits Tumor Necrosis Factor-{alpha}-Induced Reactive Oxygen Species Generation, Transcription Factor Activation, and Cell Adhesion Molecule Expression in Human Aortic Endothelial Cells. Arterioscler Thromb Vasc Biol. 2003; 23(9):1559-1566
[80] Bagchi D, Bagchi M, Stohs SJ, Das DK, Ray SD, Kuszynski CA, Joshi SS, Pruess HG. Free radicals and grape seed proanthocyanidin extract: importance in human health and disease prevention. Toxicology. 2000;148(2-3):187-197
[81] Young JF, Dragsted LO, Daneshvar B, Lauridsen ST, Hansen M, Sandstrom B. The effect of grape-skin extract on oxidative status.Br J Nutr. 2000;84(4):505-513
[82] Guerra MC, Speroni E, Broccoli M, Cangini M, Pasini P, Mingett A, Crespi-Perellino N, Mirasoli M, Cantelli-Forti G, Paolini M. Comparison between Chinese medical herb Peuraria lobata crude extract and its main isoflavone puerarin antioxidant properties and effects on rat liver CYP-catalased drug metabolism. Life Sci 2000;67(24):2997-3006
[83] Allen SJ, Gan Q, Matthews R, Johnson PA. Comparison of optimised isotherm models for basic dye adsorption by kudzu. Bioresour Technol. 2003;88(2):143-152
[84] Rezvani AH, Overstreet DH, Perfumi M, Massi M. Plant derivatives in the treatment of alcohol dependency. Pharmacol Biochem Behav. 2003;75(3):593-606
[85] Guerra MC, Speroni E, Broccoli M, Cangini M, Pasini P, Minghett A, Crespi-Perellino N, Mirasoli M, Cantelli-Forti G, Paolini M. Comparison between chinese medical herb Pueraria lobata crude extract and its main isoflavone puerarin antioxidant properties and effects on rat liver CYP-catalysed drug metabolism. Life Sci. 2000;67(24):2997-3006
[86] Kvasnicka F, Biba B, Sevcik R, Voldrich M, Kratka J. Analysis of the active components of silymarin. J Chromatogr A. 2003;990(1-2):239-245
[87] Shimizu I. Antifibrogenic therapies in chronic HCV infection. Curr Drug Targets Infect Disord. 2001;1(2):227-240
[88] Dhanalakshmi S, Agarwal P, Glode LM, Agarwal R. Silibinin sensitizes human prostate carcinoma DU145 cells to cisplatin- and carboplatin-induced growth inhibition and apoptotic death. Int J Cancer. 2003 Sep 20;106(5):699-705].
[89] Gruenwald J, Brendler T, Jaenicke C, ed. PDR for Herbal Medicine, 2 nd ed. Medical Economics, Montvale (NJ) 2000
[90] Kurowska EM, Dresser G, Deutsch L, Bassoo E, Freeman DJ. Relative bioavailability and antioxidant potential of two coenzyme q10 preparations. Ann Nutr Metab. 2003;47(1):16-21
[91] Lu H, Liu GT. Anti-oxidant activity of dibenzocyclooctene lignans isolated from Schisandraceae. Planta Med 1992;58(4):311-313
[92] Boileau TW, Liao Z, Kim S, Lemeshow S, Erdman JW, Clinton SK. Prostate carcinogensis in N-methyl-N-nitrosourea (NMU) testosterone-treated rats fed tomato powder, lycopene, or energy restricted diets. J Natl Cancer Inst 2003;95(21):1578-1586
[93] Chainani-Wu N. Safety and anti-inflammatory activity of curcumin: a component of tumeric. J Altern Complement Med. 2003;9(1):161-168
[94] Gehman JM. From the Office of the President: Pseudo-Group Once Again Misleading the Naturopathic Field. Official Bulletin ANA, January 25, 1948:7-8
[95] Rouhi AM. Escorting metal ions: protein chaperone protects, guides, copper ions in transit. Chem Eng News, 1999;11:34-35
[96] Himelblau E, et al. Identification of a functional homolog of the yeast copper homeostasis gene ATX1 from Arabidopsis. Plant Physiol 1998;117(4):1227-1234
[97] Adams AK, Best TM . The Role of Antioxidants in Exercise and Disease Prevention. Physician & Sportsmed, 2002;30(5):37-46
[98] Hardy G, Hardy I, Ball PA. Nutraceuticals – a pharmaceutical viewpoint: part II. Curr Opin Clin Nutr Metab Care. 2003;6(6):661-71
Some of these studies (or citations) may not conform to peer review standards. Therefore, the results are not conclusive. Professionals can, and often do, come to different conclusions when reviewing scientific data. None of these statements have been reviewed by the FDA. All products distributed by Doctors’ Research, Inc. are nutritional and are not intended for the treatment or prevention of any medical condition.













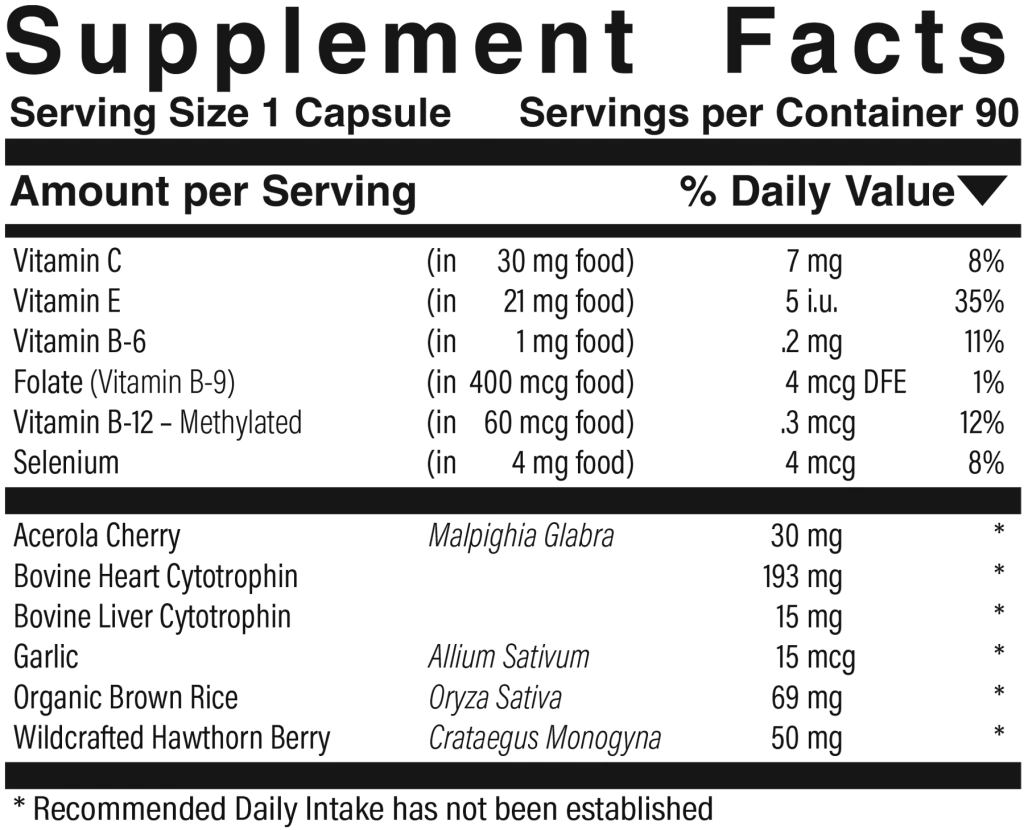
 Vitamin-Mineral™ $40.00
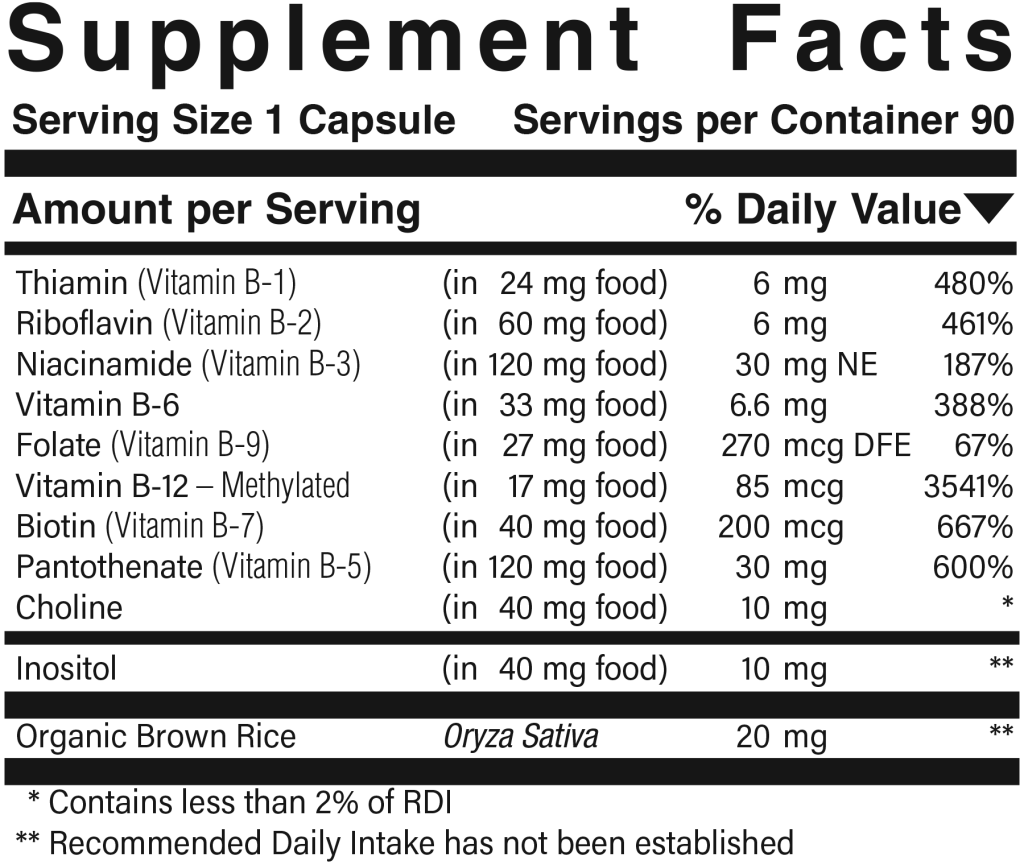
Vitamin-Mineral™ $40.00 B Stress Complex™ $40.00
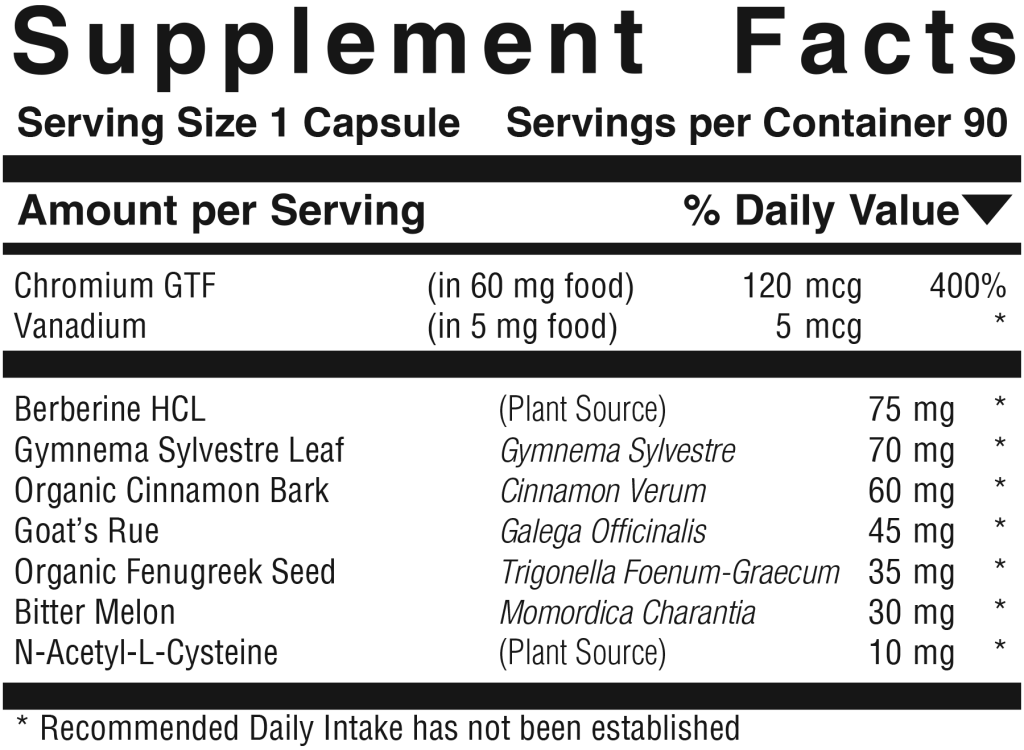
B Stress Complex™ $40.00 Gluco-Sugar-Balance™ $37.00
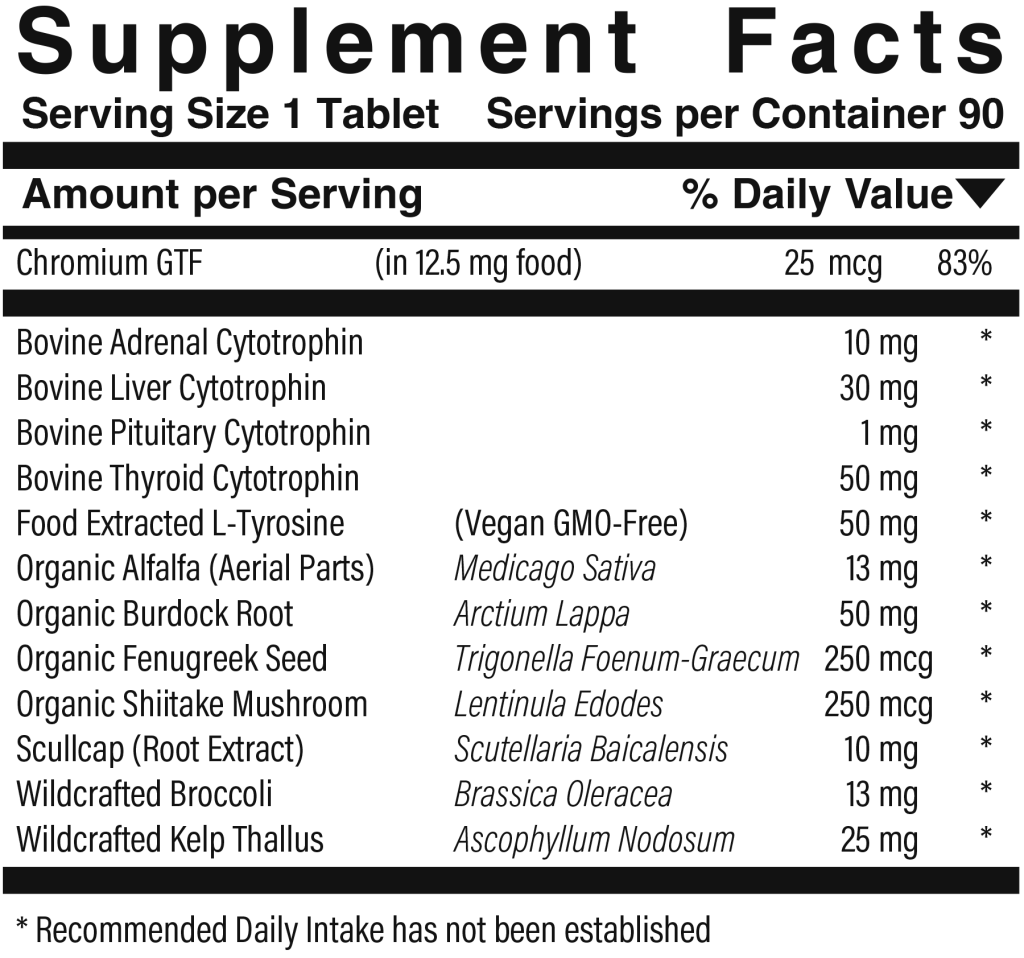
Gluco-Sugar-Balance™ $37.00 Metabolic Thyro™ $28.00
Metabolic Thyro™ $28.00